- repetitive compression or rubbing of the tendons (mainly supraspinatus) under coraco-acromial arch i.e. subacromial space
- during abduction -> conjoint tendon slides under coraco-acromial arch
- abduction approaches 90 deg -> subacromial space narrows
- internal rotation -> narrower, external rotation -> wider
- naturally, at 90 deg abduction -> arm externally rotates to increase the space
- activities with repeated int. and ext. rotation (window cleaning, wall painting) -> compression, rubbing, friction of the tendon -> impingement syndrome
- Impingement Position -> abduction, slight flexion, internal rotation
- Site of impingment -> critical area of diminished vascularity in the supraspinatus tendon about 1 cm proximal to its insertion into the greater tuberosity
Intrinsic factors
- degeneration of the tendon (age-related, cell-mediated)
- changes in the presence of highly sulphated glycosaminoglycans
- changes in the collagen composition with loading.
- Changes in vascularity
All these changes -> rotator cuff dysfunction -> upward displacement of the humeral head -> subsequent extrinsic compression.
Extrinsic factors
- spurs growing down the coracoacromial ligament
- a laterally sloping acromion
- osteoarthritic thickening of the acromioclavicular joint
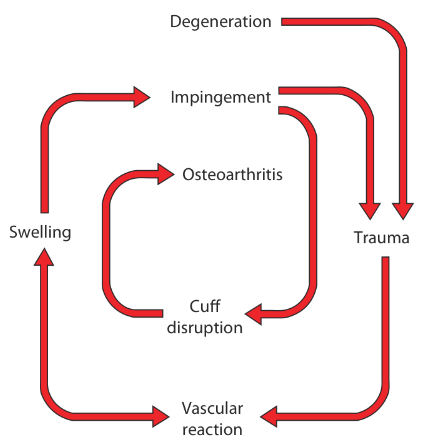
Effects
- friction -> tendinitis (edema, swelling) -> usually self-limiting
- prolonged / repetitive -> minute tears -> scarring, fibrocartilaginous metaplasia, calcification in the tendon
- healing -> vascular reaction -> local congestion -> narrowing of the space -> further impingement
- slow healing / sudden strain -> microscopic tear extends -> partial / full thickness tear -> loss of abduction
- large tears -> disturbed shoulder mechanics -> osteoarthritis of the glenohumeral joint
Clinical features
- typically those of a Rotator Cuff Syndrome
- Subsequent progress depends on the
- stage of the disorder,
- the age of the patient and
- the vigour of the healing response
- 3 patterns
- subacute tendinitis
- chronic tendinitis
- cuff disruption
Subacute tendinitis (painful arc syndrome)
- anterior shoulder pain after vigorous/unaccustomed activity
- tenderness along the anterior edge of acromion (easily elicited on extension)
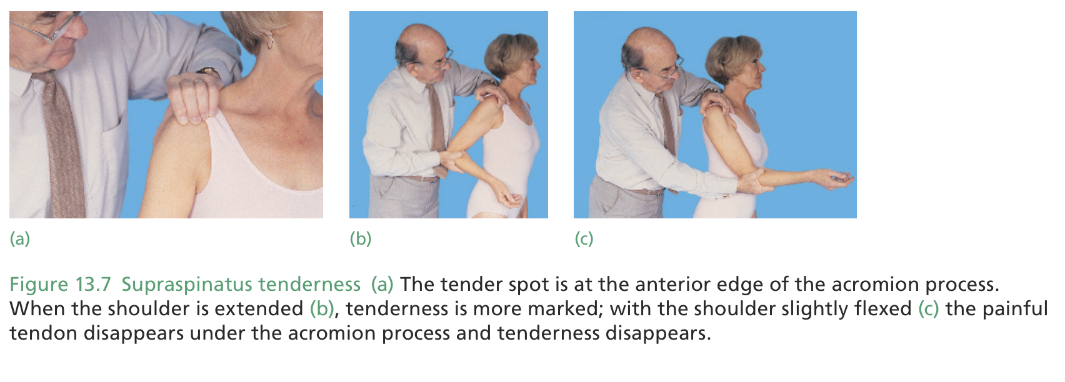
- often reversible, relieves spontaneously by activity modification
Chronic tendinitis
- recurrent attacks of subacute tendinitis
- pain relieves with rest, anti-inflammatory treatment
- recurs with more demanding activity
- pain is worse at night, patient cannot lie on the affected side
- pain restricts even simple activities like hair grooming, dressing
- signs of bicipital tendinitis (tenderness in the bicipital groove, crepitus on moving tendon)
Most advanced stage is progressive fibrosis and cuff disruption. Patient gives history of refractory shoulder pain, increasing stiffness and weakness.
Partial tear
- remaining fibers allow active abduction with a painful arc
- difficult to differentiate from chronic tendinitis
Complete tear
- active abduction is not possible even after local anesthetic injection
- initially passive abduction is limited by pain, later passive abduction is full
Tests for impingement pain
- The painful arc
On active abduction, pain aggravates between 60 and 120 degrees.
Pain lessens when abduction is done with full external rotation. - Neer’s impingement sign
- stabilize the scapula with one hand
- raise the arm to full extent in passive flexion, abduction and internal rotation
- positive -> pain in the subacromial space or anterior edge of acromion
- sensitivity 80%, poor specificity
- also positive in acromioclavicular osteoarthritis, glenohumeral instability and SLAP lesions.
- Neer’s test for impingement
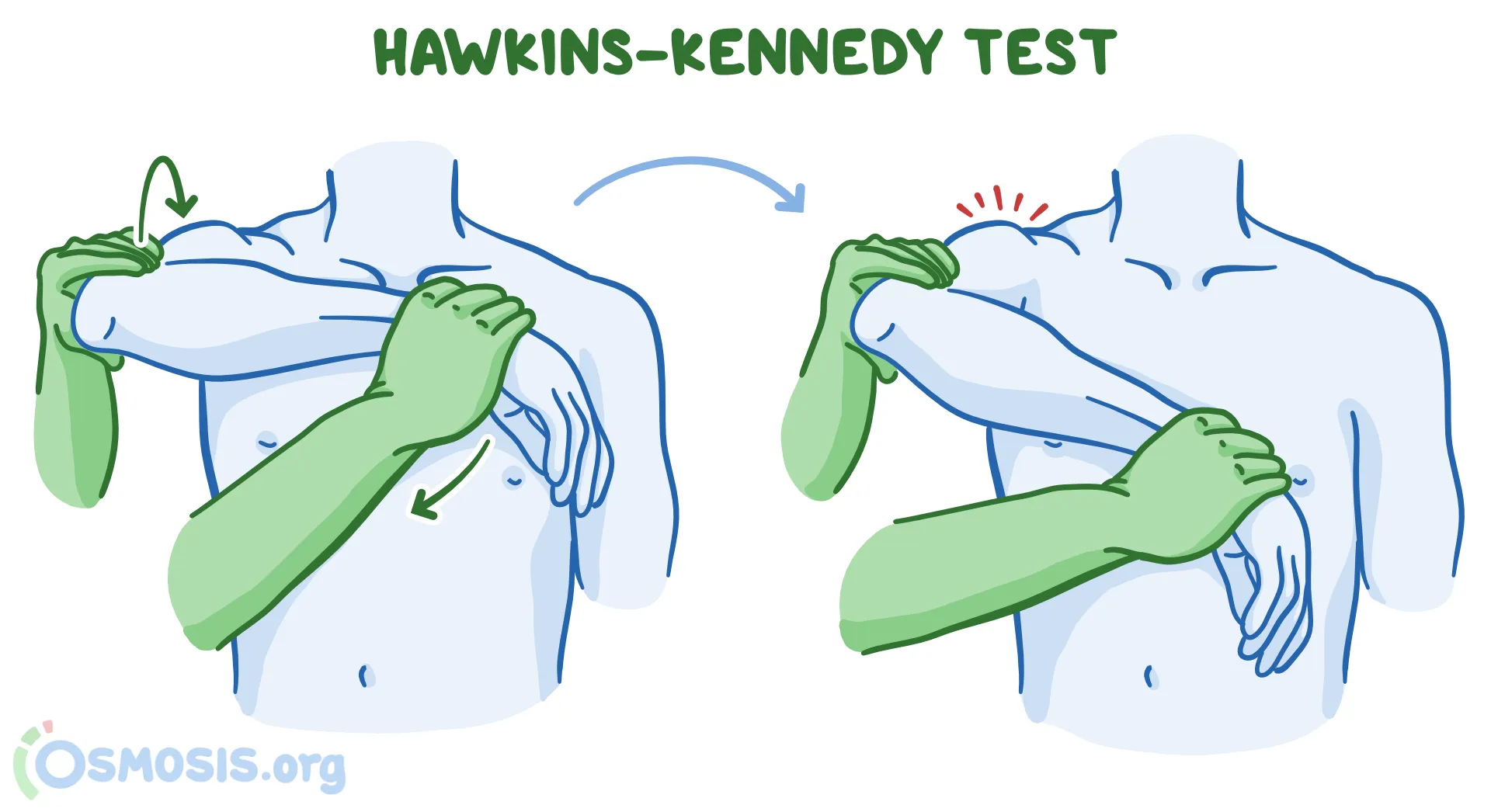
If the previous test is positive, repeat it after injecting 10 mL of 1% lignocaine (i.e. 5 mL of 2%) into the subacromial space. If pain goes away, it confirms the diagnosis - Hawkin’s Kennedy test
- Arm elevated to 90 degrees, elbow flexed to 90 degrees
- stabilize the arm & internally rotate it
- positive -> pain around the anterolateral aspect of shoulder
- highly sensitive, poorly specific
- Jobe’s test
- arm elevated and internally rotated, elbow extended, thumb pointing to the ground
- patient is told to hold this position, while the examiner puts downward pressure
- pain indicates supraspinatus irritation
- weakness (i.e. inability to hold the position) indicates supraspinatus tear
Tests for isolated weakness
- supraspinatus - empty can test (Jobe’s)
- infraspinatus - resisted external rotation
- subscapularis - belly press test, lift-off test
- infraspinatus and posterior cuff - lag sign, drop sign
Imaging
- X-ray
- early stage -> normal
- chronic tendinitis -> there may be erosion, sclerosis or cyst formation at the site of cuff insertion on the greater tuberosity
- in caudal tilt view -> roughening or overgrowth of the anterior edge of the acromion, thinning of the acromion process and upward displacement of the humeral head
- features of osteoarthritis in acromio-clavicular and gleno-humeral joint
- MRI
- effectively demonstrates the structures around the shoulder
- up to 1/3 of asymptomatic individuals have abnormalities of the rotator cuff on MRI.
- Changes on MRI need to be correlated with the clinical examination.
- Ultrasonography
- accuracy is comparable with MRI
Treatment
Conservative
- uncomplicated impingement is often self-limiting
- teach patients how to avoid the impingement position
- physiotherapy (see Rehabilitation Protocol for Rotator Cuff Tendinitis)
- short course of NSAID
- if all these fail & before disability becomes marked -> 1-2 intra-articular steroid injections in the subacromial space + protective modification of shoulder activity for at least 6 months
Surgical
- Acromioplasty
- Rotator cuff repair
both can be done in open or arthroscopic method