History#
- History of ovulation inducing drugs or use of ART
- Family history of twinning
Symptoms#
- Increased nausea & vomiting
- Unusual rate of abdominal enlargement
- Excessive fetal movement
Signs#
General Examination#
- Anemia (more than singleton pregnancy)
- Unusual weight gain
- Evidence of pre-eclampsia
Abdominal Examination#
Inspection#
- Abdomen is unduly enlarged
Palpation#
- Height of the uterus is more than the period of amenorrhea
- Girth of the abdomen is more than the normal average at term (100 cm)
- Palpation of too many fetal parts
Auscultation#
- Simultaneous auscultation of 2 distinct heart sounds
Investigation#
- USG of the pregnancy profile
Treatment#
Antenatal Management#
- Increased dietary supplement (extra 300 calories)
- Increased rest
- Early cessation of work
- Increased supplementation of iron, vitamins, calcium, folic acid
- More frequent antenatal visit
- USG every month
- Hospitalization if any complications or at 38 weeks of pregnancy
Obstetric Management#
First Stage of Labor#
- Skilled obstetrician and neonatologist should be present
- Patient should be in bed (to prevent early rupture of the membranes)
- Careful monitoring
- One bag of blood should be kept in hand
- Check for cord prolapse if membrane ruptures
Delivery of the First Baby#
- Same guidelines as normal labor
- Liberal episiotomy
- Don’t give IV ergometrine after delivery
- The baby is labeled as number 1
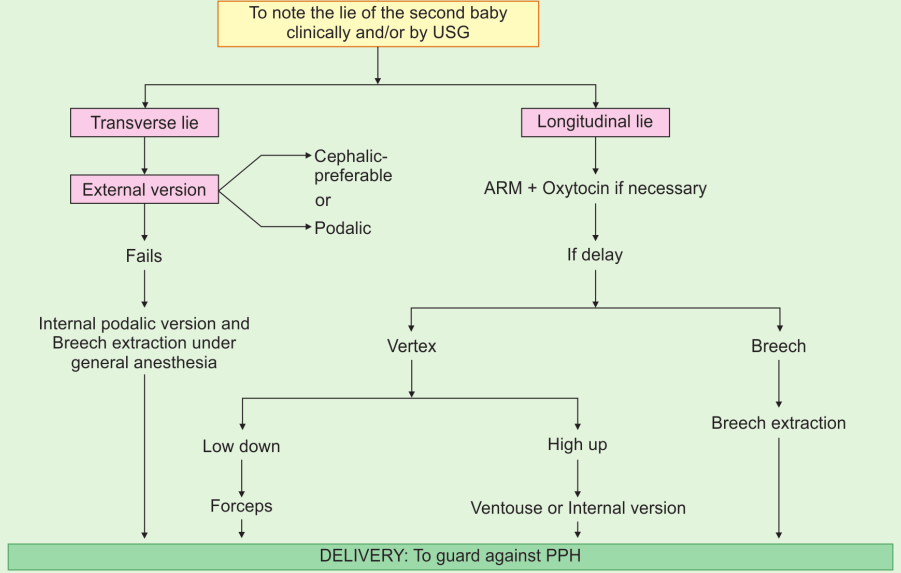
Delivery of the Second Baby#
Complications#
Maternal#
During Pregnancy#
- Anemia
- Hyperemesis gravidarum
- Pre-eclampsia
- Polyhydramnios
- Preterm labor
- Antepartum hemorrhage
- Malpresentation
During Labor#
- Early rupture of membranes
- Cord prolapse
- Prolonged labor
- Intrapartum hemorrhage
During Puerperium#
- Postpartum hemorrhage
- Puerperal sepsis
- Subinvolution
Fetal#
- Prematurity
- Twin-twin transfusion syndrome
- Discordant twin growth
- Intrauterine death (IUD) of one fetus
- Conjoined twins
- Locked twins
- Perinatal asphyxia
- Stillbirth